Ocrelizumab: A Friendly, Science-Backed Guide for People Living With MS
If you’ve heard of ocrelizumab (brand name often used in clinics), you probably know it’s a “B-cell depleting” therapy given twice a year. But what does the best scientific evidence actually show—about benefits, side effects, vaccines, pregnancy, and the new subcutaneous option? Let’s walk through it together, minus the jargon and the scare-caps.
1 How ocrelizumab works (in plain English)
Ocrelizumab is a laboratory-made antibody that seeks out CD20-positive B cells—immune cells that help drive multiple sclerosis activity—and temporarily reduces their numbers. Fewer misbehaving B cells typically means fewer relapses and less new inflammatory activity in the brain and spinal cord. It’s used in relapsing forms of MS and—importantly—the first therapy shown to slow disability in primary progressive MS (PPMS). The pivotal trials used 600 mg every 24 weeks.
2 How well does it work?
Relapsing MS: robust benefits in head-to-head trials
 In two large studies (OPERA I & II), ocrelizumab beat interferon beta-1a (a standard therapy at the time) on pretty much every major measure. It cut the annualized relapse rate by ~46–47%, reduced disability progression, and dramatically suppressed new MRI lesions. That’s not “kinda good”—that’s “this changes my calendar” good.
In two large studies (OPERA I & II), ocrelizumab beat interferon beta-1a (a standard therapy at the time) on pretty much every major measure. It cut the annualized relapse rate by ~46–47%, reduced disability progression, and dramatically suppressed new MRI lesions. That’s not “kinda good”—that’s “this changes my calendar” good.
A systematic review and network meta-analysis comparing many MS drugs also ranked ocrelizumab among the most effective options for lowering relapse rate and disability progression, with a safety profile comparable to other treatments. Translation: even when the field gets crowded, it stays near the top.
Primary progressive MS: the first therapy with proven impact
In the ORATORIO trial (PPMS), ocrelizumab reduced the risk of confirmed disability progression at 12 weeks (hazard ratio 0.76) and 24 weeks (HR 0.75) versus placebo. People on ocrelizumab also had less MRI lesion volume increase and slower brain atrophy. That’s huge for a form of MS that historically had very few options.
Does starting earlier matter?
A long-term follow-up of the PPMS study showed that people who started ocrelizumab earlier had better outcomes over ~6.5 study-years than those who switched later: lower rates of progression on multiple measures and a smaller proportion requiring a wheelchair. Early, continuous treatment mattered.
3 Safety: what decades of data say (and what to watch)
The “greatest hits” of side effects
The most common reactions are infusion/injection reactions (usually mild-to-moderate) and infections—mainly of the upper respiratory or herpes family. Serious infections are uncommon but can happen, so clinicians monitor closely. Long-term pooled analyses up to ~7 years show a generally consistent safety profile with no new major safety signals.
Malignancy signal: where things stand
Early trials noted a numerical imbalance in cancers (notably breast cancer), which triggered careful surveillance. Pooled longitudinal data hasn’t demonstrated a clear increase above expected background rates, but vigilance remains part of routine care discussions. In short: talk risks/benefits with your team; the overall long-term safety profile is considered acceptable in the context of MS benefits.
Hepatitis B: screening isn’t optional
B-cell–depleting therapies can allow dormant hepatitis B to wake up (reactivate). Case reports in MS on ocrelizumab underline this risk—so universal HBV screening before starting and monitoring during treatment is standard. If you’ve ever had hepatitis B (or aren’t sure), raise it early.
Immunoglobulins (antibodies) and infection risk
Over time, some people develop low immunoglobulin levels—most often IgM, occasionally IgG. Real-world cohorts report that hypogammaglobulinemia is not always tied to serious infections, but clinicians still keep an eye on it with periodic lab checks.
4 Vaccines, COVID-19, and timing (yes, timing matters)
Routine, non-live vaccines
In the VELOCE study, people on ocrelizumab mounted weaker—but still present—antibody responses to standard non-live vaccines (e.g., tetanus, influenza, pneumococcal). The practical takeaway is to organize vaccines before starting if possible and maintain regular immunizations during therapy with realistic expectations.
COVID-19 vaccines
Multiple studies show that anti-CD20 therapies blunt the antibody (humoral) response to mRNA COVID-19 vaccines, while T-cell responses are often preserved. Longer time since the last infusion and some B-cell reconstitution improve vaccine responses—so clinicians frequently time boosters midway between doses when feasible.
5 Pregnancy, breastfeeding & babies
Pregnancy data in MS is better than it used to be—but still not perfect. Emerging registry analyses suggest no major new safety signals for pregnancy outcomes with anti-CD20 exposure, but because the drug crosses the placenta in later pregnancy, temporary B-cell reductions have been reported in some exposed newborns. That doesn’t mean harm is inevitable, but it does mean coordinated planning (and neonatal monitoring) is smart. Please discuss timelines, contraception, and breastfeeding with your neurology and obstetric teams.
6 Dosing & formats: IV—and now SC
Most trial evidence and current practice use 600 mg every 24 weeks by IV infusion. A phase 3 study of a subcutaneous (SC) formulation found non-inferior drug exposure and similar efficacy/safety profiles to IV, offering a quicker, HCP-administered alternative in some settings. Your clinic’s logistics and your preferences will guide the choice.
7 Practical tips to get the most from therapy
Before you start
- Make sure you’ve had hepatitis B screening and are up-to-date on non-live vaccines; get them in before the first dose when possible.
While on treatment
- Keep routine labs (including immunoglobulins) and infection-prevention habits.
- Time routine vaccinations between infusions for better responses when possible.
Family planning
- If pregnancy is in your near future, loop in neurology + OB early to map timing and neonatal monitoring if exposure occurs.
Friendly reminder: This article is educational—not personal medical advice. Decisions should be made with your healthcare team, considering your disease activity, MRI, lifestyle, and values.
8 FAQs (evidence-based, concise)
Does ocrelizumab slow disability?
Yes. It reduced disability progression in relapsing MS versus interferon and in PPMS versus placebo, with benefits sustained in long-term follow-up.
Will I still respond to vaccines?
Usually yes, but less so than without B-cell depletion. Timing doses and boosters helps; non-live vaccines are recommended.
Is cancer risk higher on ocrelizumab?
Current pooled data do not show a clear increase above expected background, but surveillance continues and shared decision-making is key.
What infections worry clinicians most?
Common ones (respiratory, herpes) plus special attention to hepatitis B reactivation if you’ve had prior infection; hence universal screening.
Is there a shot (not infusion) version?
An SC option with non-inferior exposure and similar outcomes has been studied; availability depends on your region and clinic setup.
Conclusion: the bottom line
Ocrelizumab is one of the heavy hitters against MS inflammation—cutting relapses, calming MRI activity, and slowing disability in both relapsing disease and PPMS. Long-term data support a consistent safety profile, but you and your clinician should plan around vaccines, screen for hepatitis B, and keep up with labs. If you’re considering pregnancy, start the conversation early. With the growing evidence base (and an SC option studied), you have more ways than ever to tailor therapy to your life.
- Hauser SL, et al. N Engl J Med. 2017;376:221–234. doi: 10.1056/NEJMoa1601277.
- Montalban X, et al. N Engl J Med. 2017;376:209–220. doi: 10.1056/NEJMoa1606468.
- Wolinsky JS, et al. Lancet Neurol. 2020;19:998–1009. doi: 10.1016/S1474-4422(20)30342-2.
- Hauser SL, et al. Neurology. 2021;97:e1546–e1559. doi: 10.1212/WNL.0000000000012700.
- Bar-Or A, et al. VELOCE. Neurology. 2020;95:e1999–e2008. doi: 10.1212/WNL.0000000000010380.
- Apostolidis SA, et al. Nat Med. 2021;27:1990–2001. doi: 10.1038/s41591-021-01507-2.
- Capuano R, et al. J Neurol. 2022;269:6185–6192. doi: 10.1007/s00415-022-11296-4.
- Nobile S, Beauchemin P. Can J Neurol Sci. 2024;1–8. doi: 10.1017/cjn.2024.21.
- Ciardi MR, et al. Open Forum Infect Dis. 2019;6(1):ofy356. doi: 10.1093/ofid/ofy356.
- McCool R, et al. Mult Scler Relat Disord. 2019;29:55–61. doi: 10.1016/j.msard.2018.12.040.
- Newsome SD, et al. OCARINA II SC OCR. Neurology. 2025;104(9):e213574; erratum 2025;105(3):e213909. doi: 10.1212/WNL.0000000000213574.
- Van Kempen ZLE, et al. J Neurol Sci/MSARD/related (representative longitudinal vaccine data). doi examples within cohort literature.
- Brill L, et al. JAMA Neurol. 2021;78(12):doi: 10.1001/jamaneurol.2021.3599 (anti-CD20 vaccine responses).
- Vukusic S, et al. Pregnancy outcomes on anti-CD20. Neurol Neuroimmunol Neuroinflamm. 2024. doi: 10.1212/NXI.0000000000200349.
- Khoo B, et al. Pediatrics. 2025; e2025070891 (neonatal B-cell cytopenia after in utero exposure). doi: 10.1542/peds.2025-070891
Related Articles
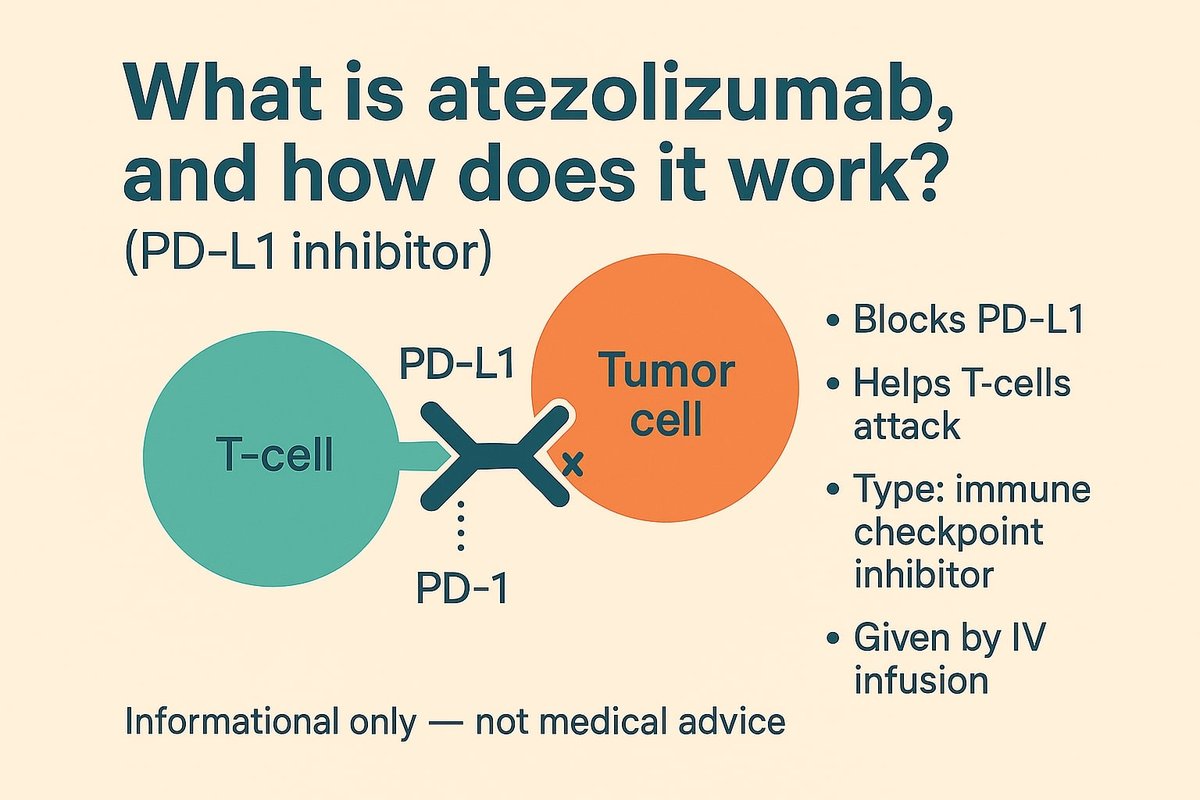
Atezolizumab (Tecentriq): A Plain-English Guide Backed by Science
Atezolizumab (Tecentriq) is a PD-L1–blocking immunotherapy used across several cancers. This guide …
Daratumumab: What It Is, How It Works, and Why It’s a Big Deal
Daratumumab is the first anti-CD38 antibody to reshape multiple myeloma care. Here’s what it does, …
Mepolizumab: What the Science Says (and Why Your Eosinophils Care)
Mepolizumab, a targeted anti-IL-5 antibody, can cut exacerbations and steroid use in eosinophilic d…